

Why COVID mask mandates were possibly dangerous and almost certainly unethical, part 2
Why COVID mask mandates were possibly dangerous and almost certainly unethical, part 2


This post is a sequel of part 1. See part 1 here.
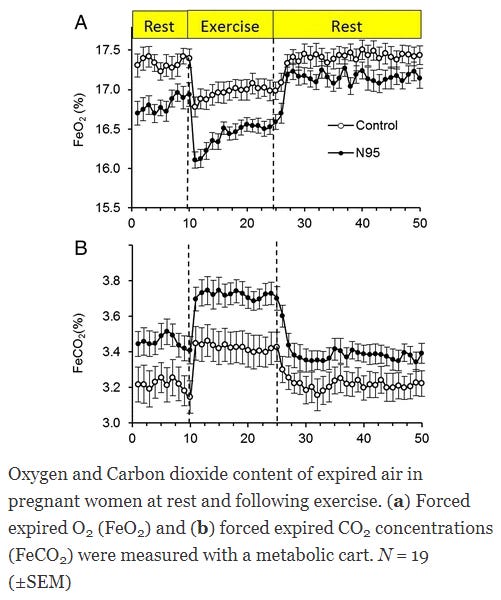
Below are some of the data showing the physiological—and in some cases health—impact of masking in pregnant women.
First, here is a study conducted in pregnant women using N95s, looking at exhaled O2 and CO2. It clearly shows an impact of the N95s on these exhaled gases. N95 wearers exhale more CO2 and less O2.
Second, confirming this effect is this remarkable paper, showing an increase in red blood cells in women during the period of heavy mask use in Israel. It also showed that such women had decreased platelets and increased rates of post-partum hemorrhage. This is consistent with a large body of literature showing that chronic hypoxia induces a reduction in platelet counts (here but also elsewhere). Such data in particular suggest that chronic masking may lead to a higher risk of bleeding.
This study is a confirmation of the above data because it demonstrates a robust physiological compensation to low blood oxygen, that spans across not just hemoglobin but even platelets.
However, we do not have any good experimental (RCT-level) evidence in pregnant women (or, in the parlance of the present era: birthing people) of the long-term effects of mask-wearing and therefore no strong evidence that these effects occur in women.
All we have are animal studies, a clear indication that changes in CO2 concentrations do occur in mask-wearing women, and a suggestion that this may lead to functional effects, such as an increased propensity toward postpartum hemorrhage.
What other effects might there be? We don’t know.
It therefore seems reasonable to say, given this evidence gap, that benefits to mask-wearing should be clearly demonstrated to justify mandates.
We will return to this.
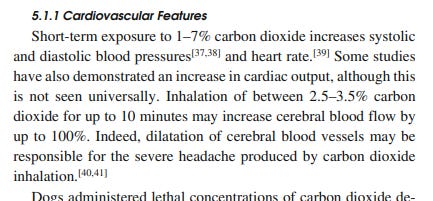
Let's loop back to the beginning. We mentioned that cognitive impairment occurred at just 0.15% CO2 in a substantial body of human research.
Yet as we have seen in the masking studies, inhaled CO2 can exceed 3%.
Is there any evidence that masking can impair cognition?
One recent study suggests that there is: it showed that chess players wearing masks made significantly worse decisions.
This is consistent with evidence showing that high CO2 concentrations impair decision-making processes.
This finding is confirmed in this abstract, showing that prolonged masking modestly impaired cognition.

Other, more short-term studies found no significant effect, which may be due to the duration of mask-wearing and its impact on oxygenation.
Surveys confirm these findings among healthcare workers. In one survey of 343 nurses during the Covid pandemic, more than 90% reported adverse effects after wearing an N95 respirator on shift.

Headache was by far the most common adverse effect reported, which is believed by researchers in the field to be caused by dilation of the brain's blood vessels in response to elevated CO2--the same mechanism by which caffeine withdrawal causes headache.
Back to the paper. Skin breakdown was also remarkably common among these nurses. As was acne.

Yet a full quarter of nurses also reported noticeably impaired cognition, consistent with what we saw reported above.

Another study among healthcare workers showed similarly high rates of adverse effects among operating room workers, with these increasing over time. By 4 hours, the majority of workers (70%) had some adverse effects.

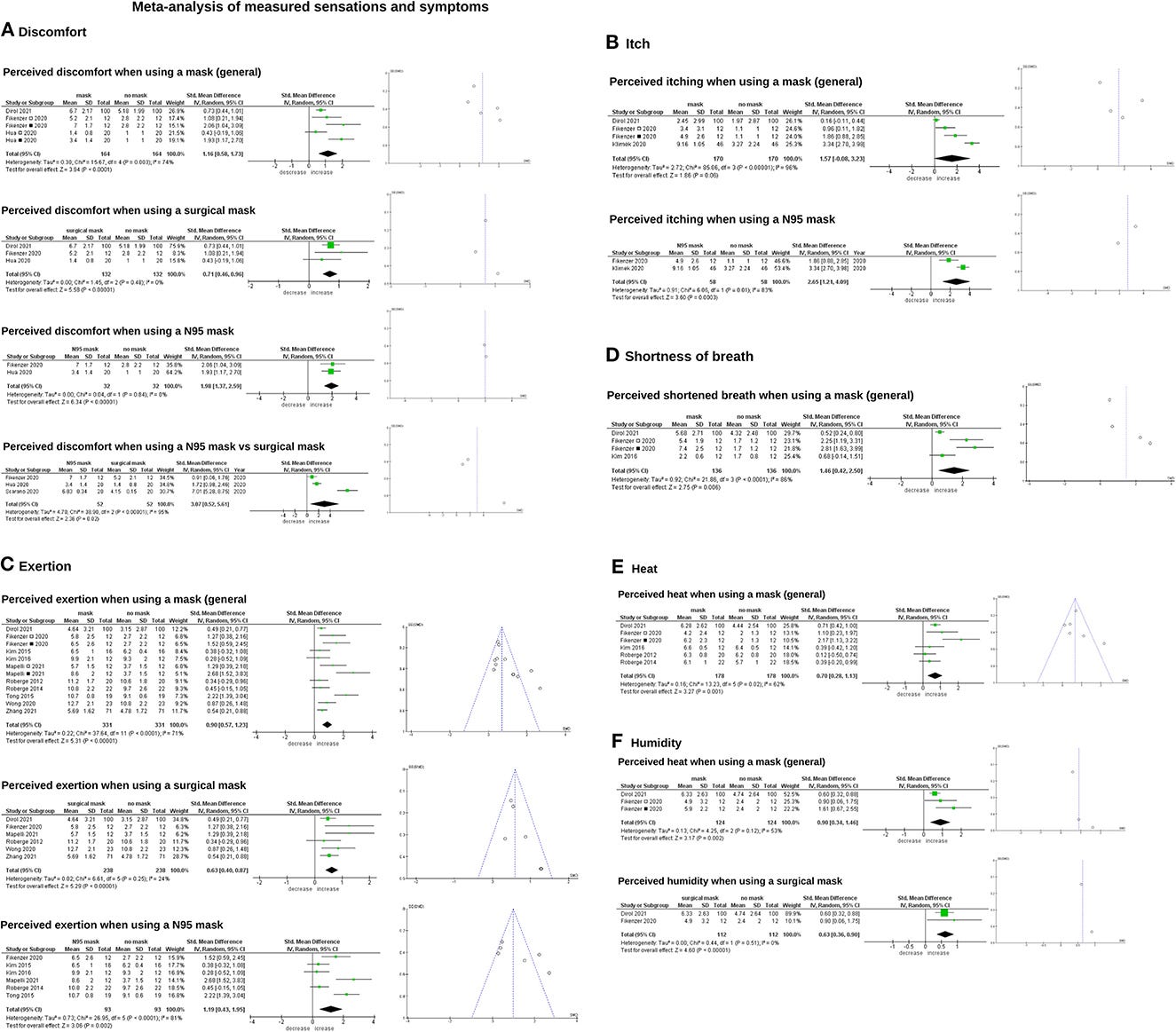
This brings us to a recent meta-analysis published on the topic.
It showed:
Increased blood oxygenation
Increased blood and exhaled CO2
Increased heart rate
Increased blood diastolic and systolic pressure
Increased risk for:
Difficulty breathing
Discomfort
Headache
Acne
Skin irritation
Voice disorder
Dizziness
And much more
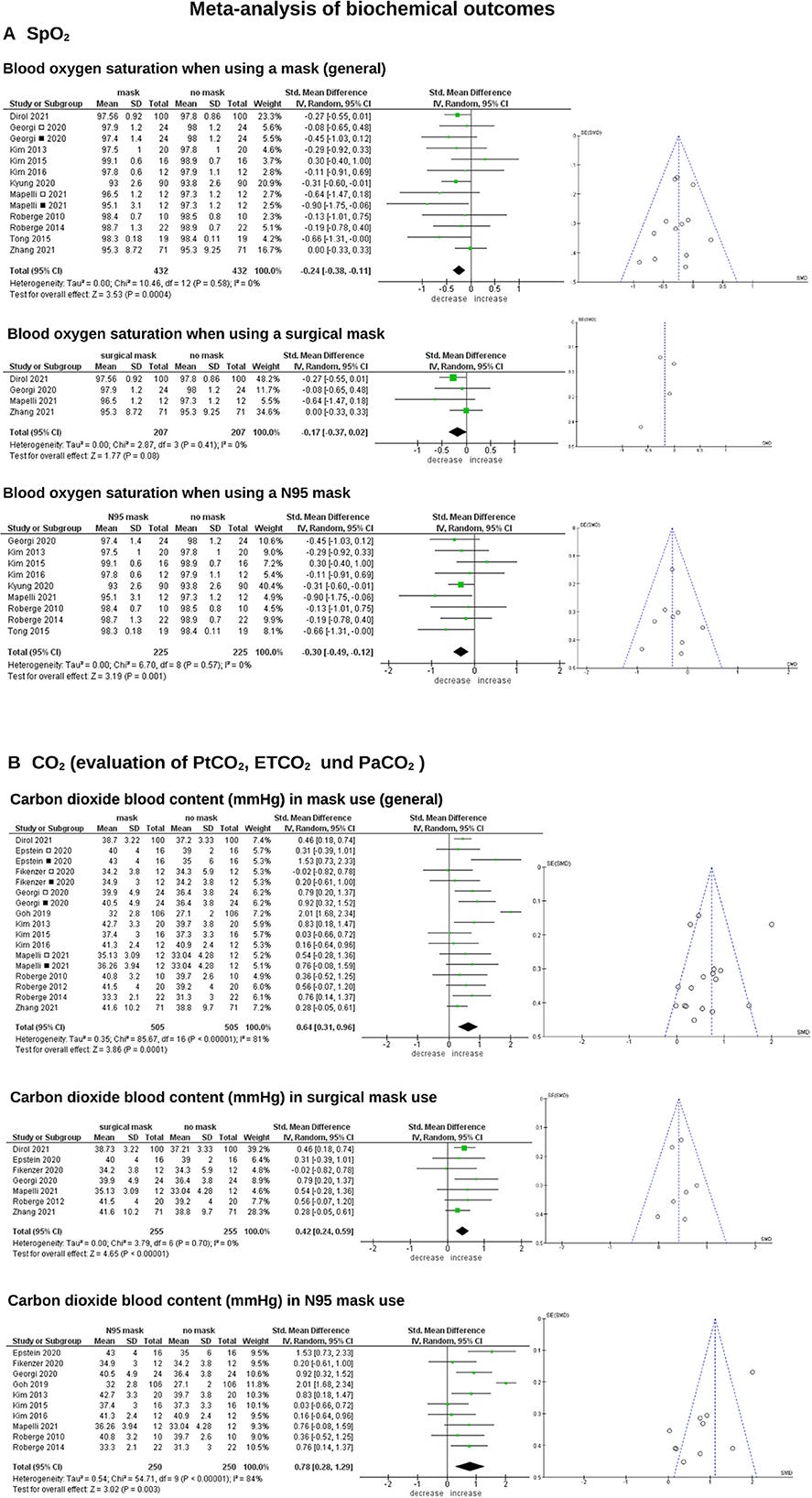

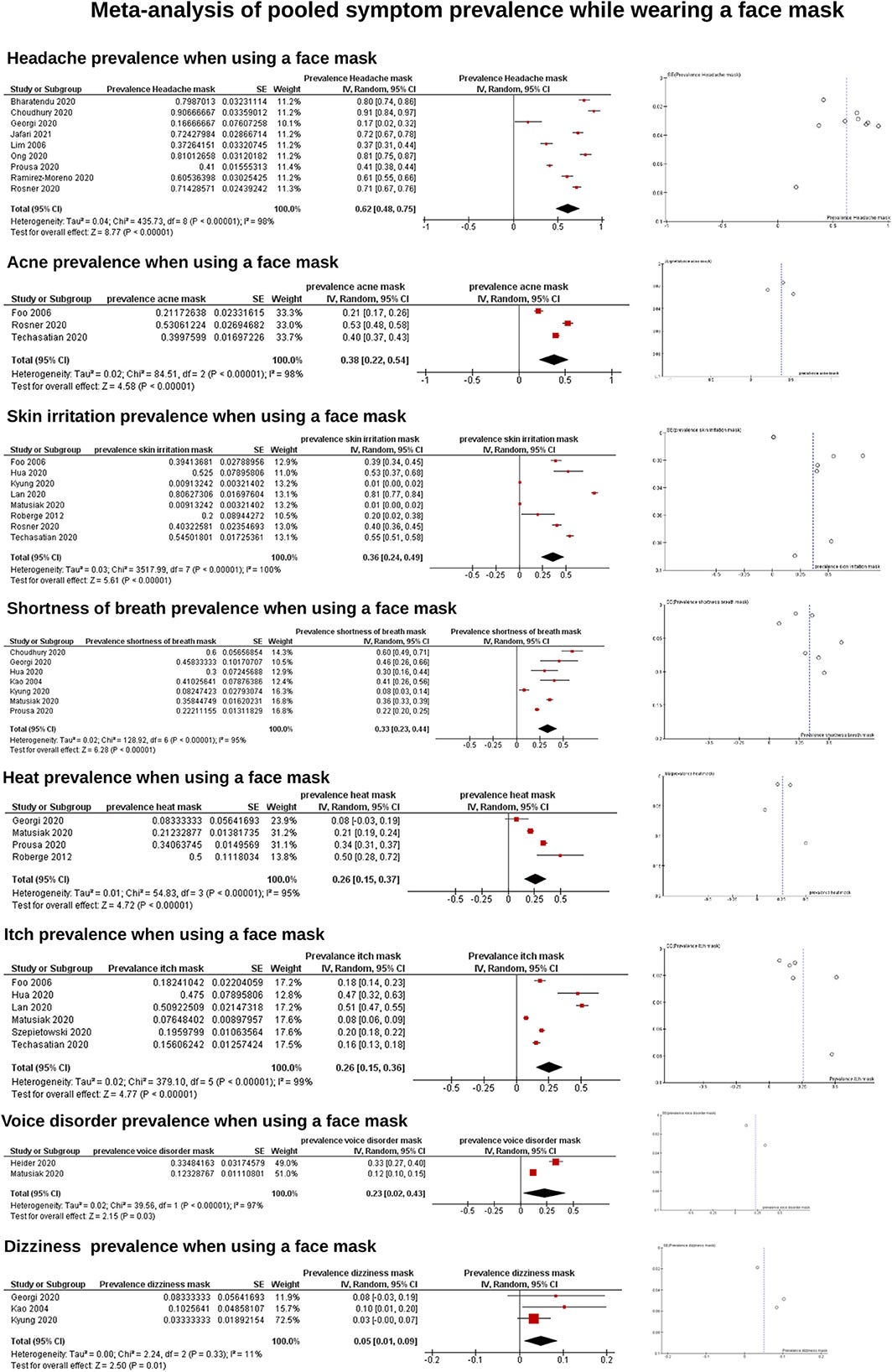
Most criticisms of this study online focused on the SpO2 reading changes, but the other outcomes were more important since they actually affected the experience of subjects.
The findings in the above meta-analysis are consistent across a wide variety of research publications and are not really disputable.
The question is really only how big the negative effects of masking are, in which contexts they occur, and which effects are common and which are more rare.
As a side note, the modest impact of surgical masking on SpO2 can be gleaned by just a passing familiarity with the masking literature. Here is a figure from a study.

Yes, masking does reduce O2, modestly. But the CO2 effects are much more important.
This brings us to the final and most important point.
Only two of sixteen randomized controlled trials on masks for infection prevention have shown modest benefits.
Meta-analysis, furthermore, does not show any benefit of mask-wearing for this purpose.
Why therefore, given the above documented and potential harms of masking, were mandates thought to be justified?
In Congressional testimony, CDC Director Rochelle Walensky claimed that there was no equipoise, meaning there was no debate that mask benefits exceeded harms.
However, as we have seen, harms of masking are clearly substantial and even potentially serious, while benefits are unestablished.
Why therefore were mask mandates implemented?
In short, we can speculate that this was done because pandemic policy was woke: so overwhelmed by emotional considerations, critical thinking about risks and benefits was bulldozed.
This kind of mass psychosis, thankfully, occurred only in the context of a mild pandemic and not during some other more serious event. We must take it seriously so that we do not find ourselves in a much more serious situation in the future--and behave the same irrational way.
Please sign up as a paid subscriber if you enjoy reading my work.